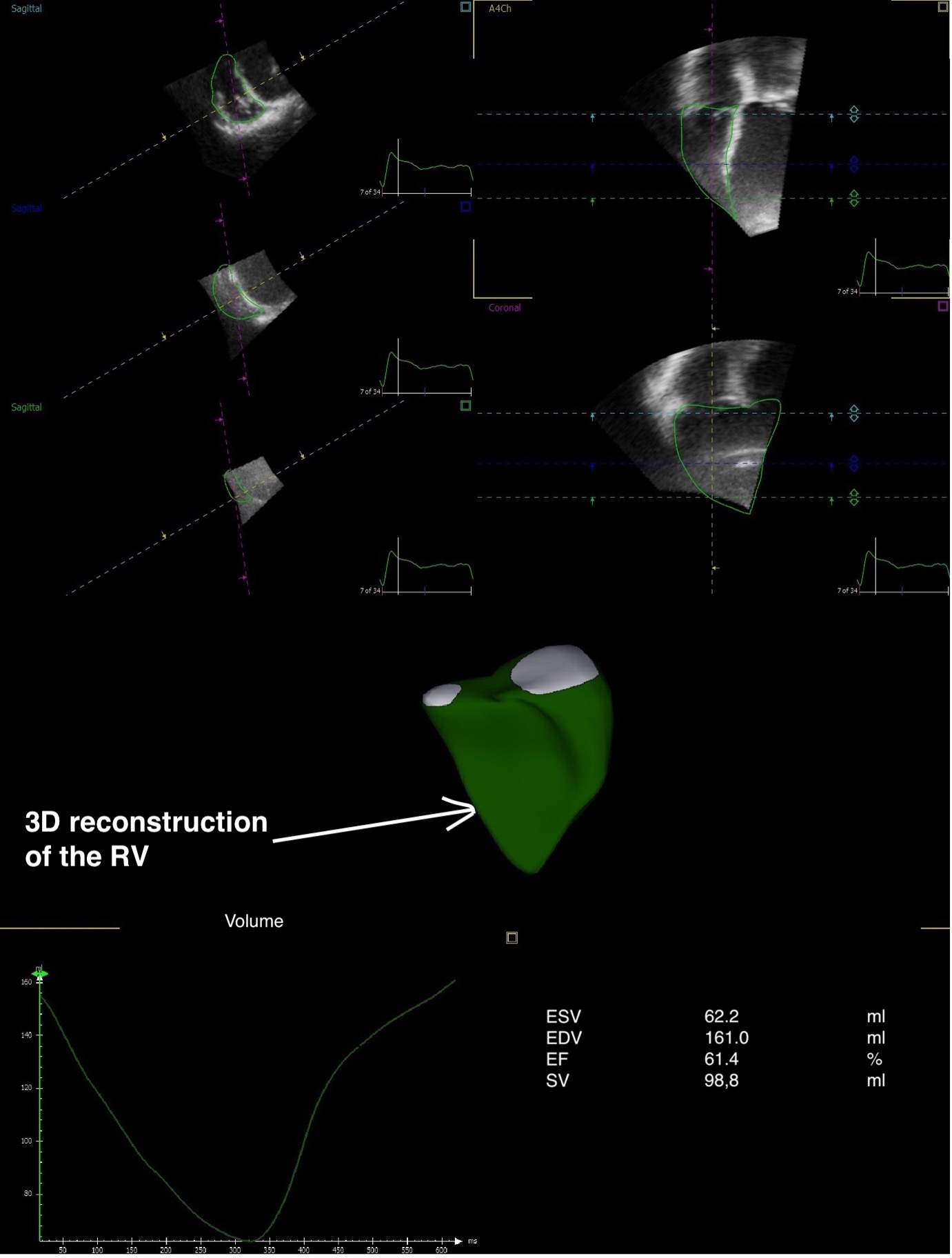
Background: Right ventricular-pulmonary artery coupling (RVPAC) is a predictor of outcome in pulmonary hypertension. However, the role of this parameter in dilated cardiomyopathy (DCM) remains to be established. The aim of this study was to assess the contribution of RVPAC to the occurrence of severe heart failure (HF) symptoms in patients with DCM using three-dimensional (3D) echocardiography. Methods: We prospectively screened 139 outpatients with DCM, 105 of whom were enrolled and underwent 3D echocardiographic assessment. RVPAC was estimated non-invasively as the 3D right ventricular stroke volume (SV) to end-systolic volume (ESV) ratio. Severe HF symptoms were defined by New York Heart Association (NYHA) class III or IV. We evaluated differences in RVPAC across NYHA classes and the ability of RVPAC to predict severe symptoms. Results: Mean left ventricular (LV) ejection fraction was 28±7%. Mean RVPAC was 0.77±0.30 and it was significantly more impaired with increasing symptom severity (p=0.001). RVPAC was the only independent correlate of severe HF symptoms, after adjusting for age, diuretic use, LV systolic function, LV diastolic function and pulmonary artery systolic pressure (OR 0.035 [95% CI, 0.004 – 0.312], p=0.003). By receiver-operating characteristic analysis, the RVPAC cut-off value for predicting severely symptomatic status was 0.54 (area under the curve=0.712, p<0.001). Conclusion: 3D echocardiographic SV/ESV ratio is an independent correlate of severe HF symptoms in patients with DCM. 3D RVPAC might prove to be a useful risk stratification tool for these patients, should it be further validated in larger studies.