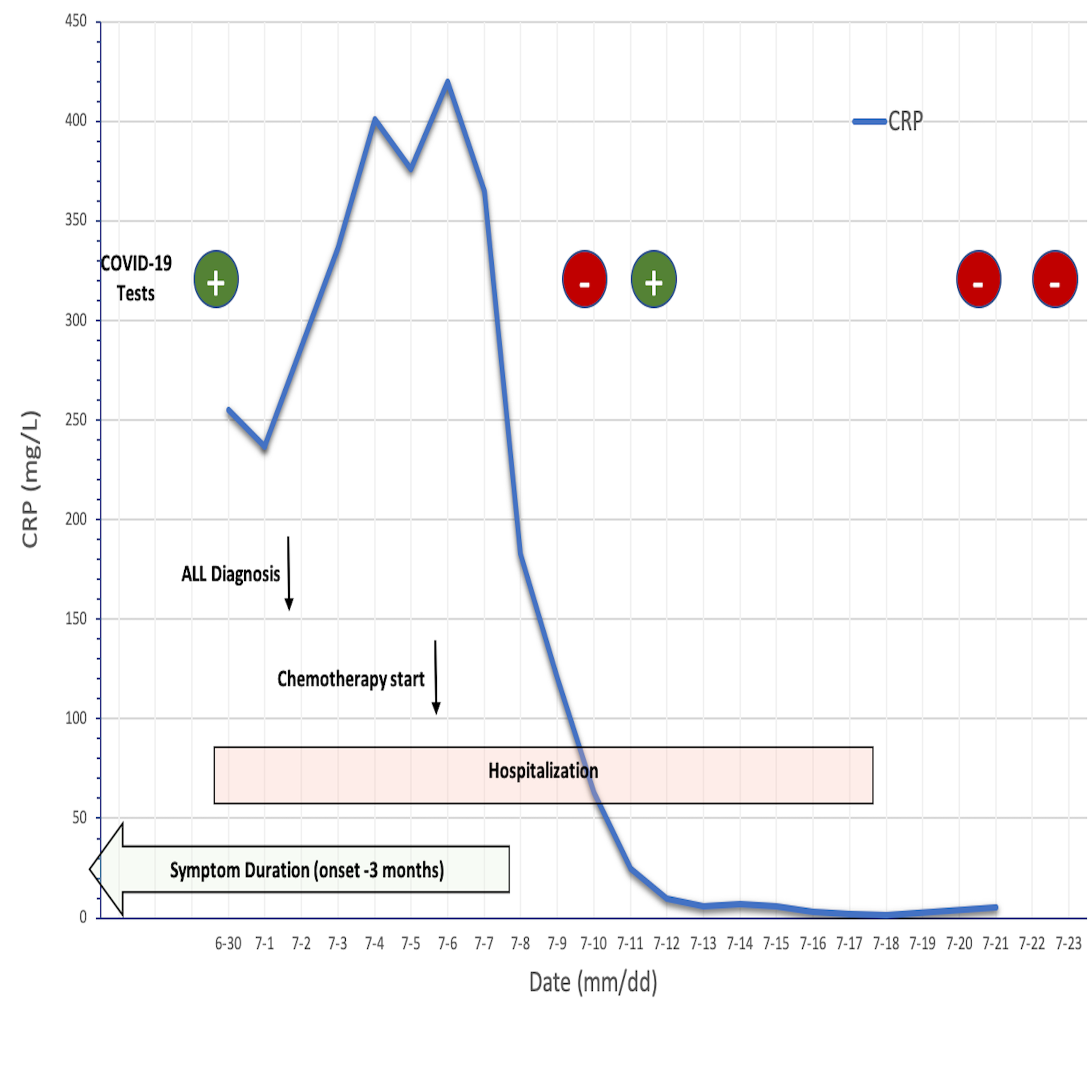
To the Editor,We read the letter entitled “Acute lymphoblastic leukemia onset in a 3-year-old child with COVID-19 ” by Marcia et al . with great interest and we hereby suggest to start chemotherapy within the same timeline as for non-COVID-19 acute lymphoblastic leukemia (ALL) patients, following our experience managing a 3-year-old boy with concomitant diagnoses of precursor B-ALL and COVID-19. The patient was a previously healthy boy who presented to our hospital with a two-month history of intermittent fevers, night sweats, fatigue and cervical lymphadenopathies. His mother had been tested positive for COVID-19 three months earlier. He had been seen by his family physician by teleconference at the onset of his symptoms, at which point a COVID-19 infection was suspected but not confirmed. The persistence of symptoms and new onset of bone pain led his parents to reconsult at our hospital. At presentation, he had no respiratory symptoms. Physical examination was remarkable for fever, tachycardia and cervical lymphadenopathies. Bloodwork revealed pancytopenia and circulating peripheral blasts. Inflammatory markers were elevated (fibrinogen 7.08 g/L; C-reactive protein 255 mg/L; sedimentation rate 63 mm/h; ferritin 185 ug/L; D-dimers 0.51 ug/ml). Capillary gas, renal function, hepatic function, coagulation studies (INR/aPTT) and cardiac biomarkers (troponin and pro-BNP) were normal. Chest radiograph (CXR) was normal. COVID-19 testing by nasopharyngeal swab was positive. Bone marrow aspiration revealed 80% precursor B lymphoblasts of hyperdiploid subtype.Patient was admitted to a dedicated COVID-19 ward. Given the absence of SARS-CoV-2 infection’s severity criteria, no COVID-19-specific treatment was initiated. Chemotherapy was started promptly once the diagnostic work-up was completed, 6 days following the patient’s confirmed COVID-19 diagnosis. The patient was treated with a three-drug chemotherapy induction based on National Cancer Institute standard-risk criteria consisting of methylprednisolone, vincristine and asparaginase. Supportive treatment consisted of intravenous hydration and allopurinol for tumor lysis prevention, empirical antibiotics, blood transfusions and prophylactic low molecular weight heparin for COVID-19-associated thromboembolic complications. The patient’s clinical course was favorable; fevers, bone pains, peripheral blasts and inflammatory markers resolved quickly following the steroid prophase. Persistent and unexplained tachycardia led to extensive investigations given concerns for COVID-19-related thromboembolic complications. Troponins, pro-BNP, electrocardiogram, echocardiography, CXR and chest CT scan were unremarkable, and the tachycardia improved with packed red blood cell transfusion. The first negative COVID-19 test was obtained on day 4 of induction therapy but came back positive 48 hours later. The patient was discharged on day 13 of induction therapy. Three consecutive nasopharyngeal swabs were negative on days 21, 23 and 38 following COVID-19 diagnosis (Fig.1). End-induction bone marrow aspiration was consistent with morphologic remission and end-induction minimal residual disease by flow cytometry was positive at 0.025%.This case demonstrates the feasibility of treating children with newly diagnosed ALL who tested positive for COVID-19, without chemotherapy delay or modification, nor specific COVID-19 treatments, as done by Marcia et al . The province of Quebec constitutes the COVID-19 epicenter in Canada with half of all Canadian cases; the prevalence of COVID-19-positive cases was 3.3% among children under the age of 10, 5.3% between the age of 10-20 years and 49.2% for people aged 50 years and above.1 Importantly, no death has been reported among children in the province of Quebec, while 97.6% of COVID-related deaths were among individuals over the age of 60 years.1 Children appear to be less affected from COVID-19 infection and exhibit a milder disease course compared to adults, although the impact of COVID-19 infection among pediatric oncology patients remains unknown.2-4 Current published recommendations in the management of pediatric oncology patients during the COVID-19 pandemic emphasize on the importance of pursuing protocol-prescribed chemotherapy regimens based on the curable nature of most pediatric malignancies and the milder COVID-19 disease course observed in the pediatric population.4 However, case reports of severe COVID-19 disease in pediatric oncology patients start to emerge,5 and management of concomitant COVID-19 infection and newly diagnosed ALL can be challenging. First, our patient presented with a multisystem inflammatory syndrome which made it difficult to discern whether he was symptomatic from the COVID-19 infection versus the leukemia itself. Furthermore, we questioned whether the positive COVID-19 test by polymerase chain reaction (PCR) amplification in our patient truly reflects active infection since there was a nearly 3-month period between the first positive test in his family and when our patient was first tested positive. The positive PCR test could result from prolonged viral shedding in an immunocompromised patient affected by his leukemia onset. Alternatively, a positive test does not necessarily indicate the presence of viable virus as Wolfel and colleagues demonstrated that virus could not be grown from samples obtained from hospitalized patients beyond the eighth day of illness.6 Therefore, the general approach to await a negative result prior to begin chemotherapy might cause significant therapy delay and adversely impact outcomes in newly diagnosed ALL patients during the COVID-19 pandemic. Indeed, our patient took over 23 days to have 2 consecutive negative PCR tests 48 hours apart. Furthermore, the use of COVID-19-specific antiviral treatment in non-critically ill children is controversial given the lack of efficacy in this population.7Antiviral treatment may have significant drug interactions with chemotherapy and contribute to additive gastrointestinal and myelosuppressive toxicities. Nevertheless, the benefit of dexamethasone in COVID-19-positive patients requiring respiratory support in reducing early mortality8 and the exquisite sensitivity of lymphoblasts to corticosteroids could be an effective early strategy to safely initiate therapy in newly diagnosed ALL patients affected with COVID-19, particularly for those presenting with oncologic emergencies such as hyperleukocytosis or mediastinal mass. As the COVID-19 pandemic continues to evolve, pediatric oncologists will be confronted with the ongoing challenge to manage newly diagnosed cancer patients with concomitant COVID-19 infection. International COVID-19 registries in pediatric oncology are actively collecting clinical data to comprehensively assess the impact of COVID-19 within this patient population and to develop standardized management guidelines.9 As for now, an assessment of risks and benefits to initiate or delay cancer therapy will need to be carefully balanced on a case-by-case basis according to the patient’s clinical symptoms, type of malignancy, evidence-based treatment options, and emerging knowledge of COVID-19’s impact in our young cancer patients.CONFLICT OF INTEREST: The authors declare no conflict of interest.REFERENCES1. INSPQ. Données COVID-190 au Québec. 2020.2. Lu X, Zhang L, Du H, et al. SARS-CoV-2 Infection in Children. N Engl J Med. 2020;382(17):1663-1665.3. Cruz AT, Zeichner SL. COVID-19 in Children: Initial Characterization of the Pediatric Disease. Pediatrics. 2020;145(6).4. Bouffet E, Challinor J, Sullivan M, Biondi A, Rodriguez-Galindo C, Pritchard-Jones K. Early advice on managing children with cancer during the COVID-19 pandemic and a call for sharing experiences. Pediatr Blood Cancer. 2020;67(7):e28327.5. Stokes CL, Patel PA, Sabnis HS, Mitchell SG, Yildirim IB, Pauly MG. Severe COVID-19 disease in two pediatric oncology patients.Pediatr Blood Cancer. 2020;67(9):e28432.6. Wolfel R, Corman VM, Guggemos W, et al. Virological assessment of hospitalized patients with COVID-2019. Nature.2020;581(7809):465-469.7. Chiotos K, Hayes M, Kimberlin DW, et al. Multicenter initial guidance on use of antivirals for children with COVID-19/SARS-CoV-2. J Pediatric Infect Dis Soc. 2020.8. Group RC, Horby P, Lim WS, et al. Dexamethasone in Hospitalized Patients with Covid-19 - Preliminary Report. N Engl J Med. 2020.9. Sullivan M, Bouffet E, Rodriguez-Galindo C, et al. The COVID-19 pandemic: A rapid global response for children with cancer from SIOP, COG, SIOP-E, SIOP-PODC, IPSO, PROS, CCI, and St Jude Global.Pediatr Blood Cancer. 2020;67(7):e28409.Figure 1. Variation of C-reactive protein (CRP) throughout the hospitalization course (blue line). COVID-19 test results are identified in green when positive and red when negative. The day of ALL diagnosis, the day of chemotherapy start (black arrows), the duration of hospitalization (red box) and the duration of symptoms (green box) are indicated. Induction chemotherapy includes: Methylprednisone/prednisone (Day 1-32), Vincristine (Day 4, 11, 18, 25), PEG-Asparaginase (Day 7) and intrathecal cytarabine (Day 1 & 18).