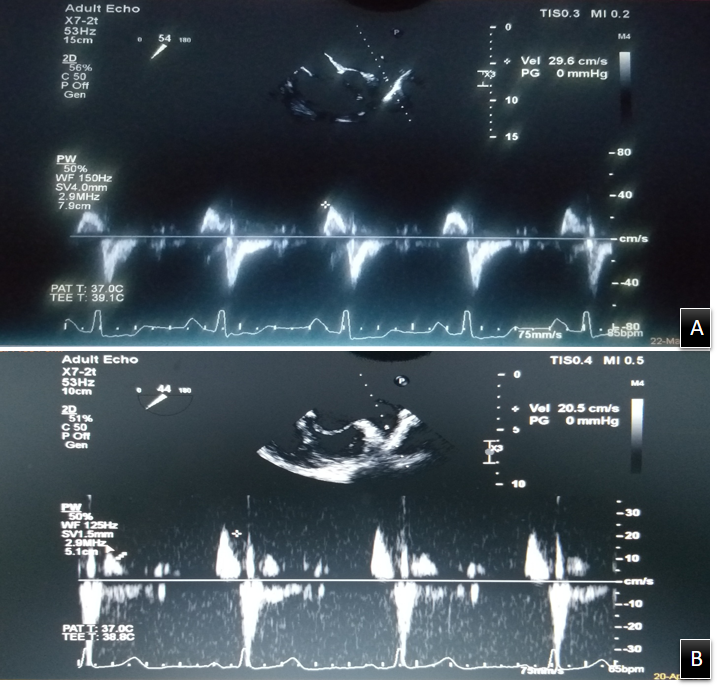
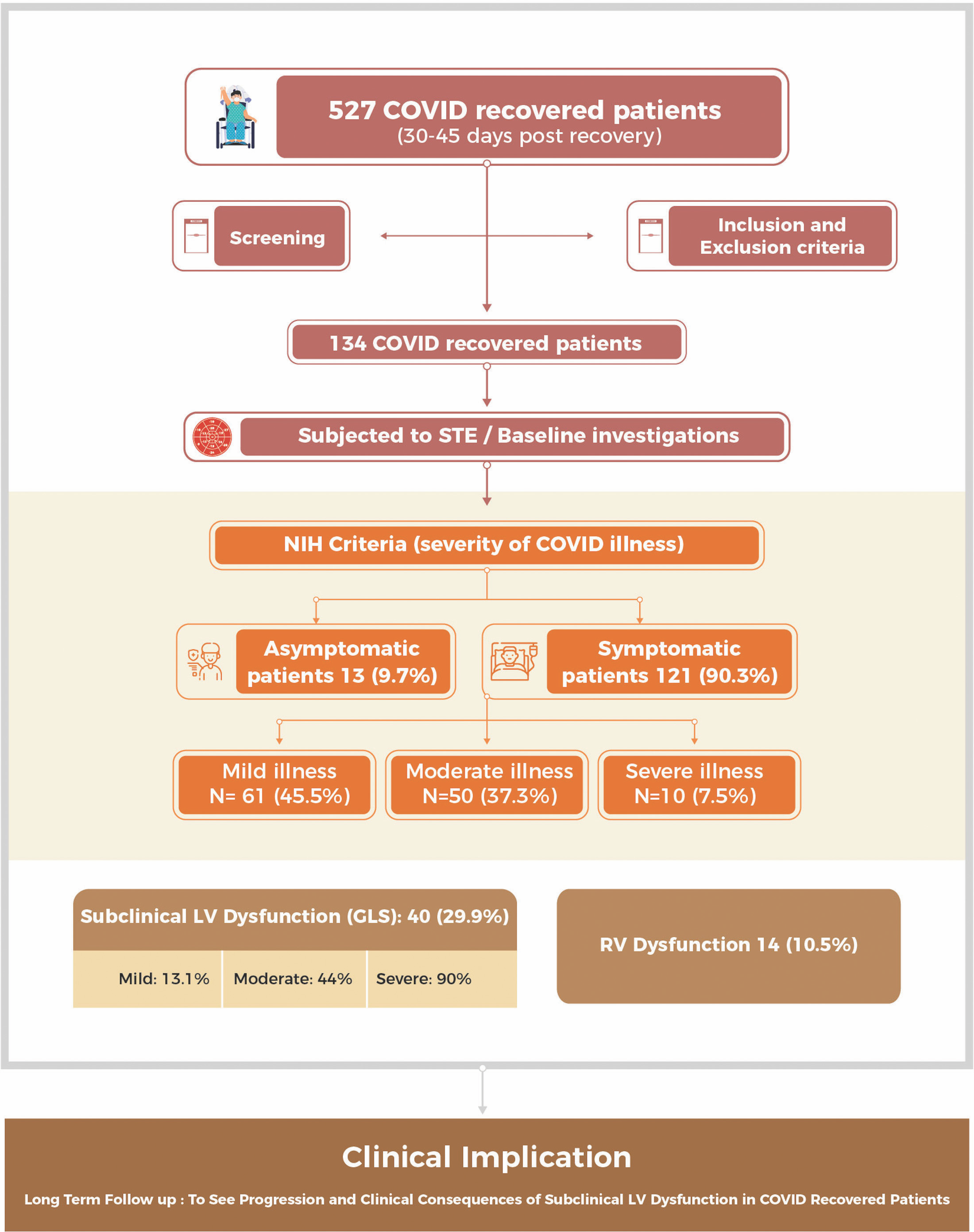
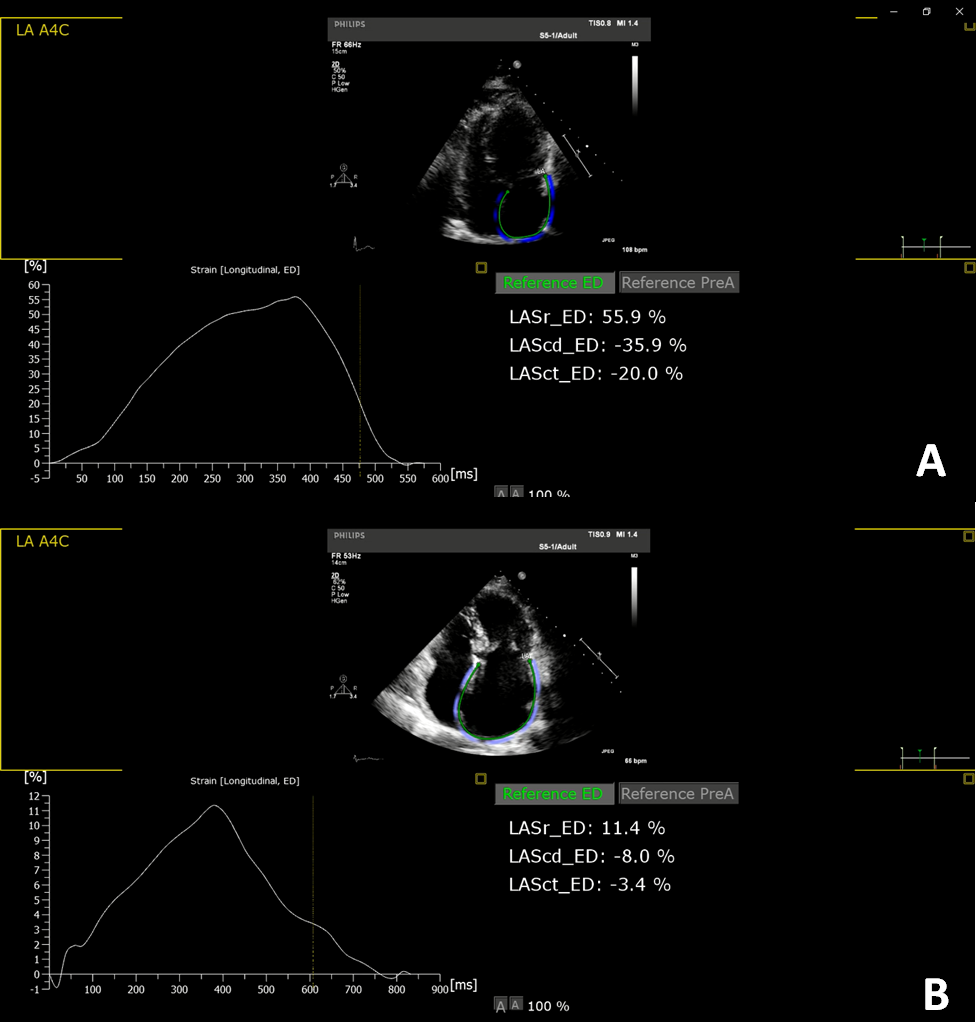
Objectives: Myocardial injury during active coronavirus disease-2019 (COVID-19) infection is well described however, its persistence during recovery is unclear. We assessed left ventricle (LV) global longitudinal strain (GLS) using speckle tracking echocardiography (STE) in COVID-19 recovered patients and studied its correlation with various parameters.Methods: A total of 134 subjects within 30-45 days post recovery from COVID-19 infection and normal LV ejection fraction were enrolled. Routine blood investigations, inflammatory markers (on admission) and comprehensive echocardiography including STE were done for all. Results: Of the 134 subjects, 121 (90.3%) were symptomatic during COVID-19 illness and were categorized as mild: 61 (45.5%), moderate: 50 (37.3%) and severe: 10 (7.5%) COVID-19 illness. Asymptomatic COVID-19 infection was reported in 13 (9.7%) patients. Subclinical LV and right ventricle (RV) dysfunction were seen in 40 (29.9%) and 14 (10.5%) patients respectively. Impaired LVGLS was reported in 1 (7.7%), 8 (13.1%), 22 (44%) and 9 (90%) subjects with asymptomatic, mild, moderate and severe disease respectively. LVGLS was significantly lower in patients recovered from severe illness (mild: -21 ± 3.4%; moderate: -18.1 ± 6.9%; severe: -15.5 ± 3.1%; P < 0.0001). Subjects with reduced LVGLS had significantly higher interleukin-6 (P < 0.0001), C-reactive protein (P = 0.001), lactate dehydrogenase (P = 0.009) and serum ferritin (P = 0.03) levels during index admission. Conclusions: Subclinical LV dysfunction was seen in nearly a third of recovered COVID-19 patients while 10.5% had RV dysfunction. Our study suggests a need for closer follow-up among COVID-19 recovered subjects to elucidate long-term cardiovascular outcomes.