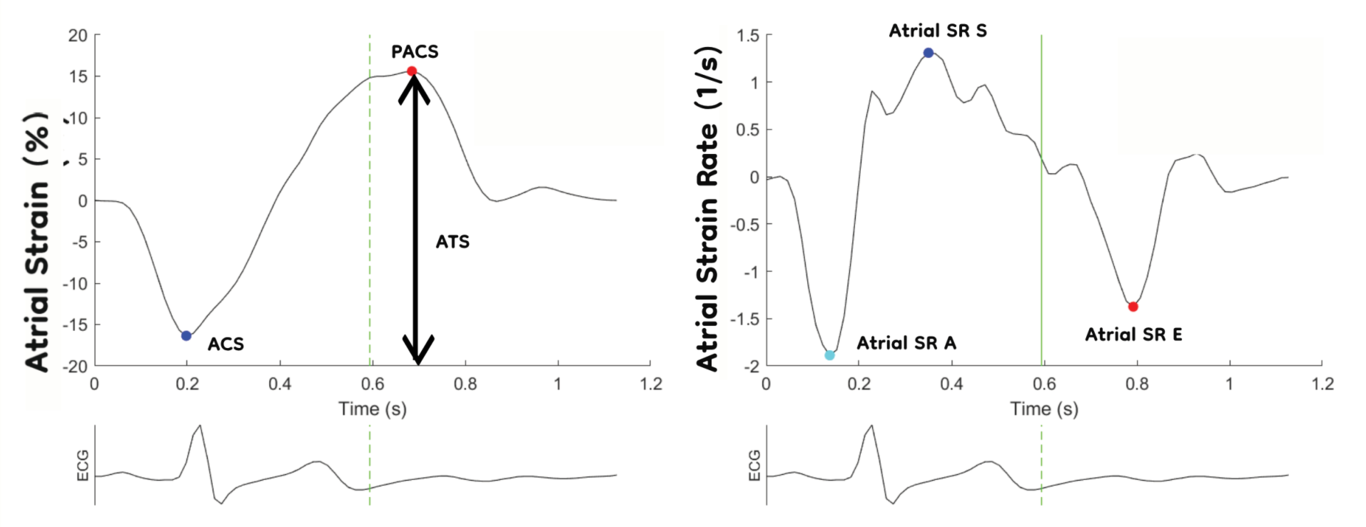
Background Noninvasive assessment of elevated filling pressure in the left ventricle (LV) remains an unresolved problem. Of the many echocardiographic parameters used to evaluate diastolic pressure, the left atrial strain and strain rate (LA S/SR) have shown promise in clinical settings. However, only a few previous studies have evaluated LA S/SR in larger populations. Methods A total of 2033 participants from Norwegian (Tromsø 7) and Russian (Know Your Heart) population studies, equally distributed by age and sex, underwent echocardiography, including atrial and ventricular S/SR and NT-proBNP measurements. Of these, 1069 were identified as healthy (without hypertension, atrial fibrillation (AF), or structural cardiac disease) and were used to define the age- and sex-adjusted normal ranges of LA S/SR. Furthermore, the total study population was divided into groups according to ejection fraction (EF) ≥50%, EF <50%, and AF. In each group, uni- and multiple regression and receiver operating characteristic curve analyses were performed to test LA and LV functional parameters as potential indicators of NT-proBNP levels above 250 ng/ml. Results The mean LA S/SR values in this study were higher than those in previous large studies, whereas the lower references were comparable. In normal hearts, atrial total strain (ATS) and mitral valve E deceleration time (MV DT) were independent factors indicating elevated NT-proBNP levels, whereas in hearts with reduced EFs, the independent indicators were peak atrial contraction strain (PACS) and LV stroke volume. The areas under the curve for these significant indicators to discriminate elevated NT-proBNP levels were 0.639 (95% confidence interval (CI): 0.577-0.701) for normal EF and 0.805 (CI: 0.675-0.935) for reduced EF. Conclusion The results confirm good intrastudy reproducibility, with mean values in the upper range of previous meta-analyses. In the future automated border-detection algorithms may be able to generate highly reproducible normal values. Furthermore, the study showed atrial S/SR as an additional indicator of elevated NT-proBNP levels in the general population, demonstrating the incremental value of both ATS and PACS in addition to conventional and ventricular strain echocardiography. Thus, the LA S/SR may be regarded as an important addition to the multiparametric approach used for evaluating LV filling.