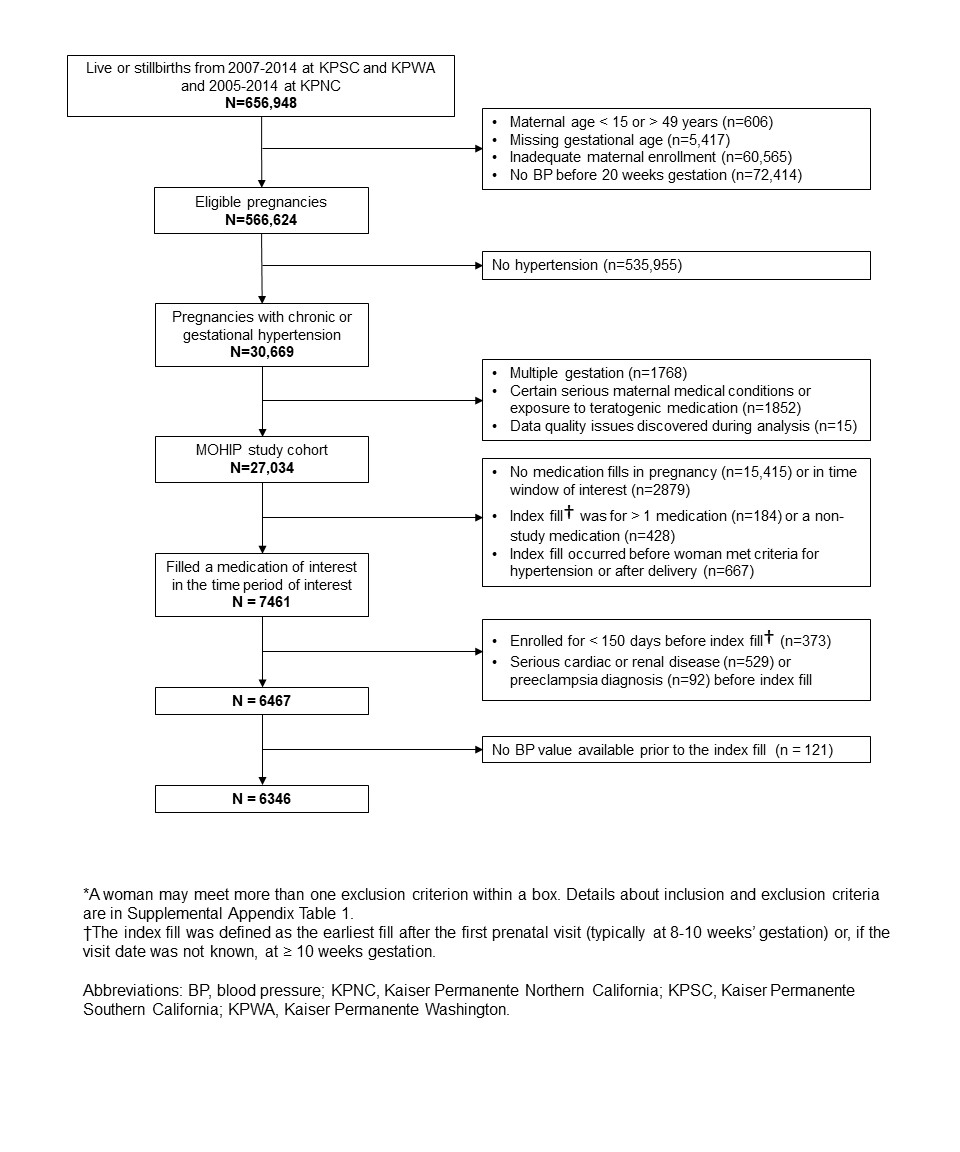
Objective: To compare maternal and infant outcomes with different antihypertensive medications in pregnancy Design: Retrospective cohort study Setting: Kaiser Permanente, a large US healthcare system. Population: Women aged 15-49 years with a singleton birth from 2005-2014 treated for hypertension. Methods: We identified medication exposure from automated pharmacy data based on the earliest dispensing after the first prenatal visit. Using logistic regression, we calculated weighted outcome prevalences, adjusted odds ratios (aORs) and 95% confidence intervals, with inverse probability of treatment weighting to address confounding. Main outcome measures: Small for gestational age (SGA), preterm delivery, neonatal and maternal intensive care unit (ICU) admission, preeclampsia, and stillbirth or termination at > 20 weeks. Results: Among 6346 deliveries, 87% with chronic hypertension, the risk of SGA (birthweight < 10th percentile) was lower with methyldopa than labetalol (prevalence 13.6% vs. 16.6%; aOR 0.77, 95% CI 0.63 to 0.92). For birthweight < 3rd percentile the aOR was 0.57 (0.39 to 0.80). Compared with labetalol (26.0%), risk of preterm delivery was similar for methyldopa (26.5%; aOR 1.10 [0.95 to 1.27]) and slightly higher for nifedipine (28.5%; aOR 1.25 [1.06 to 1.46]) and other β-blockers (31.2%; aOR 1.58 [1.07 to 2.23]). NICU admission was more common with nifedipine than labetalol (25.9% vs. 23.3%, aOR 1.21 [1.02 to 1.43]) but not elevated with methyldopa. Risks of other outcomes did not differ by medication. Conclusions: Risk of most outcomes was similar comparing labetalol, methyldopa and nifedipine. SGA risk was substantially lower for methyldopa, suggesting this medication may warrant further consideration.